
Understanding Modifier 24

Modifier 24 (Unrelated Evaluation and Management Service by the Same Physician or Other Qualified Health Care Professional During a Postoperative Period) is used when a provider performs a separately identifiable service during a patient’s post-op period.
These services are not related to the procedure previously performed. Remember the following when using Modifier 24:
- This modifier is used only with E/M services.
- It is used when the E/M service provided is unrelated to the original procedure
- It is used when the E/M service is provided by the same physician who previously performed the original procedure on the patient
- It is used when the E/M service is provided during the postoperative period of the procedure
- This modifier does not increase or decrease reimbursement. It does get the E/M service reimbursed. (Bypass edits in carrier’s software systems)
If the patient presents with a complication requiring treatment, such as bleeding or infection due to the procedure, it would be inappropriate to append the modifier.
Also remember that postoperative periods can vary from carrier to carrier and can be anywhere from 10- 90 days. Follow up visits performed outside of the global period should be coded with the appropriate E/M.

CMS to Share Physician MIPS Scores With The Public

If you were thinking of reporting the minimal amount of MIPS data to avoid a payment reduction, you might want to think again.
It has been well known that CMS publishes comparative physician data on their website (data.medicare.gov). This data in in an excel format and allows you to compare your utilization with your peers.
You MIPS data is similar to a report card and CMS will make this data available to the public on the following sites, Physician Compare, Yelp, Consumer reports and Google. The database will include individual physician names.
Publishing this data can impact the physician in a number of ways:
- Physicians looking to join new groups or selling their practice will more than likely have their scores reviewed
- Physicians who are providing excellent quality of care for their patients but elect to report only the minimum amount of data will have a lower score available to the public. This could potentially reduce the number of new patients to the practice.
It is important to keep in mind unreported measures and categories can be seen as poor performance by those who are seeking the physician’s score.

Understanding the Medicare IPPE and Annual Wellness Visits

There is a lot of confusion when it comes to the Medicare Initial Preventive Physical Examination (IPPE) and Annual Wellness Visits (AWV). Many providers document the IPPE and Annual wellness similarly to a yearly physical exam. These services are not comprehensive physicals and require a minimal physical exam. Instead, they are a tool to assess and promote the patient’s overall health and well-being. The IPPE and Annual wellness exams have different criteria. Receiving an IPPE exam does not preclude the patient from receiving an initial annual wellness.
The IPPE (G0402), commonly known as the Welcome to Medicare Visit, is eligible for new Medicare participants within their first 12 months in the Medicare plan. Medicare recommends contacting your local MAC prior to the visit to ensure the patient is eligible for the service.
The Initial AWV (G0438) is a more comprehensive visit. It is available for patients a year (at least 11 months) after their IPPE OR if the patient is no longer within the eligibility period for the IPPE. The Subsequent AWV (G0439) is an update of information received at the initial AWV.
Below is a comparison of the documentation to support each service. The items needed for both services are italicized and bold.
IPPE (G0402)
- A review of the patients medical and social history
- A review of any potential risk factors for depression/ mood disorders
- A review of the patient’s functional abilities (i.e. Hearing, ADLs, fall risk, etc.)
- A physical exam including vitals, vision acuity and any factors of concern based on the patient’s medical and social history (i.e. if the patient has cardiovascular disease the provider may examine the extremities for vascular symptoms and the heart)
- End-of-life planning
- Education, counseling and referrals based on the patient’s history, risk factors, functional ability and exam
- Treatment plan including referrals for other age based preventative services
Initial AWV(G0438)
- A Health Risk Assessment
- List of current providers and suppliers (If you are currently the patient’s only healthcare provider, that should be noted)
- A review of the patients medical and family history
- A review of any potential risk factors for depression/ mood disorders
- A review of the patient’s functional abilities (i.e. Hearing, ADLs, fall risk, etc.)
- A physical exam including vitals, and any factors of concern based on the patient’s medical and family history (i.e. if the patient’s mother had skin cancer, the provider may check for irregular moles)
- Assessment of cognitive function
- Creation of an age relevant screening schedule
- Establish a list of risk factors and any current/recommended interventions
- Advice and counseling to reduce health risks and promote wellness
It is important to note the extent of the physical examination performed is based on the patient’s medical history and either the social or family history for the IPPE and AWV. No specific diagnosis is recommended for reporting these evaluations.
Prior to these visits, it is recommended to contact the patient and/or caregiver to encourage them to bring in personal medical records, family history and a list of their current medications/ vitamins when they present for their visit.
Sources:

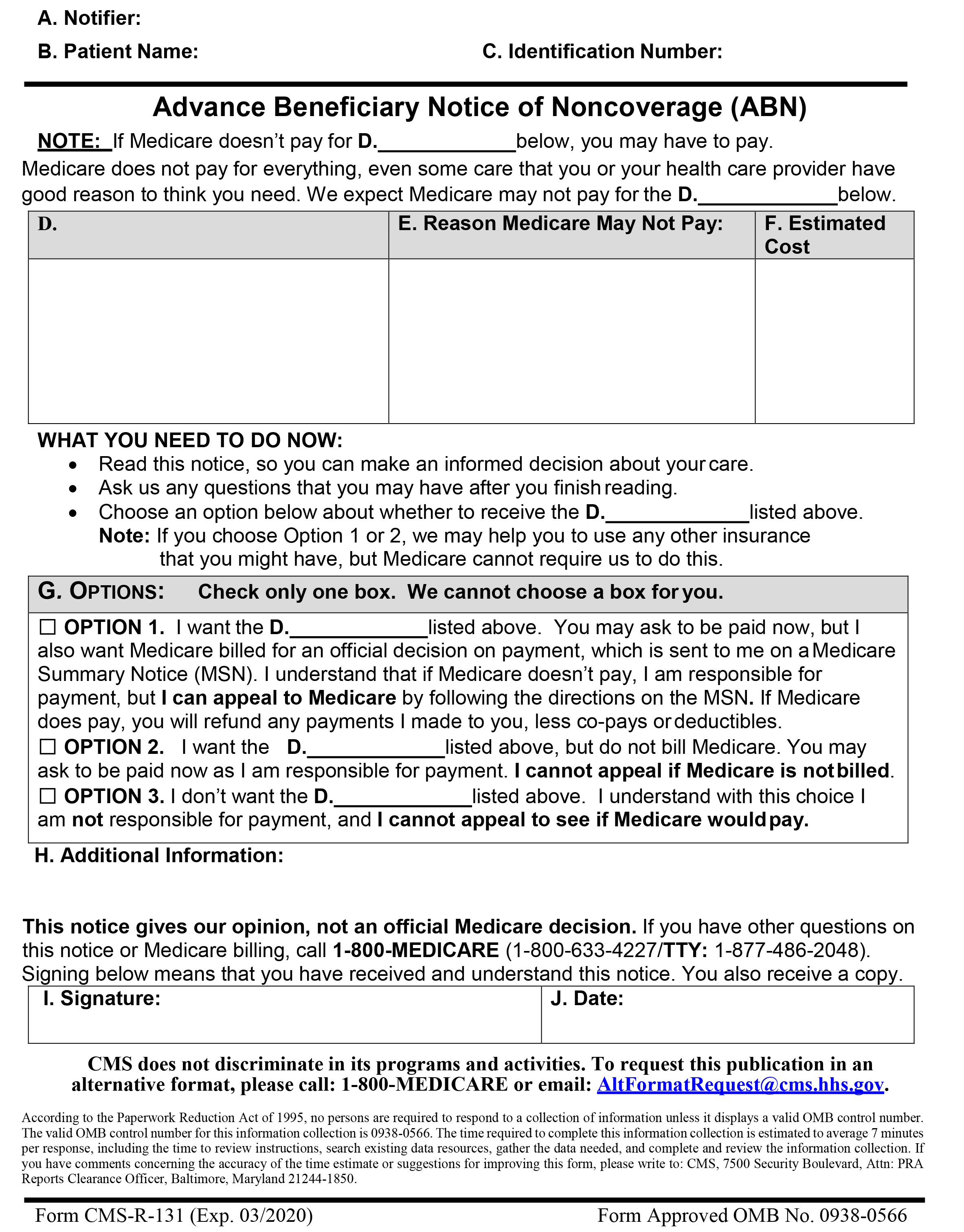
Advanced Beneficiary Notice Refresher

With the new Advanced Beneficiary Notice (ABN) coming into effect on June 21, 2017, it is a wonderful time to give a refresher on the proper way to fill out the form. ABNs are provided to educate the patient on an item/service that may not be covered by Medicare but may aid in the patient’s treatment. The ABN, when filled out properly, lets the patient know what the item / service is, when and by whom the item/service will be given /performed and the potential cost of the service. With all of the information provided, the patient can decide whether or not to have the item/service and sill sign the notice. It is important to remember without a properly filled out written notice, the patient is not financially liable if Medicare denies the item/service.
All the blanks / boxes on the form should be filled out completely. Remember to use the full names of the Notifier (supplier/treating physician) and patient. The complete item/service that will be given/performed should be entered into box “D”. For example: if the patient is going to be given physical therapy (PT) rather than writing just “physical therapy” the actual PT modalities should be noted. In Box “E” state why the service may not be paid. The estimated cost is necessary for the patient to know how much the treatment may cost if it is not covered by Medicare. Per Medicare, the estimate should be reasonable for all items/services noted. The cost should be within $100 or 25% of the fee for the item/ service. Always makes sure the patient marks the option they are choosing and the notice is signed in cursive and dated (including month, day and year).

Avoiding Obesity Counseling Denials

In 2015 Obesity Counseling G codes (G0447 Face-to-face behavioral counseling for obesity, 15 minutes and G0473 Face-to-face behavioral counseling for obesity, group (2-10), 30 minutes) were reported 240,913 times but were denied approximately 80% of the time.
There are a few key points to consider when providing and documenting for these services. First and foremost is the type of provider. The National Coverage Determination (NCD) requires the services are provided by a qualified primary care physician or other primary care practitioner in a primary care setting. The counseling can be provided by qualified auxiliary staff (e.g. dietitian) under the direct supervision of a primary care provider. Secondly these codes have a frequency limitation. • One face-to-face visit every week for the first month; • One face-to-face visit every other week for months 2-6; and • One face-to-face visit every month for months 7-12, if the beneficiary meets the 3kg (6.6 lbs.) weight loss requirement during the first 6 months.
Medlearn Matters MM7641 clearly defines the types of providers designated as primary care providers, frequency of services, and supporting diagnosis codes.
For more information on how to get it right click the following link: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM7641.pdf

Radiology Audits
Recently insurance carriers have been auditing radiology services. Some of the areas being audited you may not have even given thought to checking. For example, do the images include the initials of the technician who performed the service? Without this information, the carriers can deny the claim until the technician has been identified and their credentials verified indicting they have the required certification to perform the service.
Insurance carriers are also verifying the orders with the ordering provider to make sure the medical necessity for ordering the test is documented. In some cases, the insurance carrier is leaving that responsibility up to the servicing provider.
The source document frequently referenced by the carriers is the DOH Medicaid Update May 2006 Vol.21, No 5, Documentation Requirements for Ordered Services. Check it out https://www.health.ny.gov/health_care/medicaid/program/update/2006/may2006.htm
These are just two of the audit areas currently under review.

ICD-10-CM New/ Revised/ Deleted Code Preview Coming in Mid-April

In Mid-April we will be able to preview some of the upcoming changes to ICD-10-CM for 2018. CMS will be releasing the changes as a part of the proposed Medicare inpatient hospital payment rule. There will be fewer new, revised and deleted codes than those release for the 2017 edition.
There are several notable changes that we will be seeing in the Mid-April preview.
- New codes proposed by the American Thoracic Society (ATS) for electronic nicotine delivery systems (ENDS or e-cigarettes) will be added to Chapter 5 Mental, Behavioral and Neurodevelopmental disorders, Chapter 19 Injury, Poisoning and certain other consequences of External Causes and Chapter 21 Factors Influencing Health Status and Contact with Health Services.
- New codes for Heart Failure and Myocardial Infarction(MI) will be offering better clarity and detail for coding the different types and variety of heart failure and MIs.
- New substance abuse remission codes with explanatory information will clarify the classification for coding mild, moderate and severe. This will aid in aligning ICD-10-CM coding with the American Psychiatric Association’s Diagnostic and Statistical Manual for Mental Disorders (DSM-5).
- New Orbital roof and wall fracture codes will include greater locational specificity.
- New antenatal screening codes will be added to Chapter 21 Factors Influencing Health Status and Contact with Health Services for reporting specific screening tests administered to pregnant patients.
- We will also be seeing new explanatory language for the Glasgow coma scale to help with selecting the appropriate coding level for pediatric patients based on age.
Though it is easy to get excited about these new codes, it is important to remember the preview is a part of proposed changes. These codes, as well as others that are not yet completed, will be seen in the final hospital payment rule in August. The completed codeset with all the new, revised and deleted codes will take effect on October 1st.

NGS Changes E/M requirements for Expanded Problem Focused and Detailed Examinations
On March 16, 2017 National Government Services (NGS), a Medicare Administrative contractor (MAC), announced changes to documentation requirements for expanded problem focused and detailed examination. These changes, based on the 1995 documentation Guidelines, will make it more challenging to achieve higher levels of service for providers in in this MAC.
Under the new updates the definition of expanded problem focused and detailed exam has been updated to include more body areas/ organs systems. An “expanded problem focused” exam will be defined as 2-5 body areas or organ systems. A “detailed” exam has been changed to include 6-7 body areas or organ systems. Per NGS, the changes were made in response to provider requests for clarification on the current examination requirements.
NGS currently administers the Medicare Part A (hospital insurance) and Part B (medical insurance) contracts for the following states: Connecticut, Illinois, Maine, Massachusetts, Minnesota, New Hampshire, New York, Rhode Island, Vermont, and Wisconsin. For medical service providers in these states, the changes will be effective on July 1, 2017.