
Can I Code an Office Visit with INR Checks?

By: Lorna Simons, CPC
Medco Consultants, Inc
A quick rule of thumb is if the patient is feeling fine with no other complaints, compliant with their medication and doesn’t require changes to their current dosage, just code the prothrombin check.
As discussed in National Government Services’ 99211 Job Aid, the provider can bill out an E/M in any of the following circumstances:
- Medication management is performed
- New symptoms or side effects are evaluated (i.e. bleeding or bruising)
- Modification is made to their current therapy
- Changes are being made to the patient’s management
- Current medications are noted with the level of compliance with their medication noted.
- The provider is treating another condition or concern at the same visit
Examples:
- If a returning patient presents concerned about drinking cranberry juice while on coumadin after seeing a day time talk show “expose” and the provider then has a 10-minute discussion with the patient regarding juices and medication, the provider can code a 99212 (Established Patient E/M, straightforward complexity) with CPT code 85610 Prothrombin time.
- If a patient notes increased bruising since there last prothrombin check and the provider assesses the bruising.
- If the provider treats a URI at the same visit as the prothrombin check.
It is important to remember that all the elements of an E/M should be documented to support the E/M visit.
Source:
NGS Procedure Code 99211 Job Aid, http://ow.ly/P4C230dZECS

How To Avoid I&D Denials

By: Jacqueline Thelian, CPC, CPC-I, CHCA
Medco Consultants, Inc
Are Incision & Drainage (I&D) denials draining your wallet? Ever wonder why the insurance carrier is asking for a refund on your I&D? After all you did document “I&D done”.
Well that is the problem. Simply writing what was done without a description of the procedure, the indication for the procedure and written consent will result in a claim denial.
The CPT codes for I&D (10060-10061) are located in the surgery section of the CPT manual and as such they are designated as surgical procedures.
Let’s look at the required documentation for I&D codes 10060 & 10061.
- The signs and symptoms that required the I&D
- The pre-operative size, location and appearance of any abscess, hematoma or any lesion undergoing the I&D
- A description of the procedure to include, the equipment utilized the approximate quantity (e.g. 1cc, 5ml) and quality (e.g. serous, bloody, frank pus, etc.) of the drained material
- How the patient tolerated the procedure and any post-op instructions
- And don’t forget the signed consent, after all it is a surgical procedure.
So next time you document that I&D don’t let it drain your wallet with another denial. Use the checklist above to get it right and hold on to your reimbursement.

NGS Claim Submission Changes

By: Lorna Simons, CPC
Medco Consultants, Inc
Healthcare continues to keep up with technology with the new claim submission changes issued by National Government Services (NGS). Beginning July 10, 2017 NGS will no longer be accepting claim submissions with handwriting on the CMS 1500 form (except in the specified signature boxes). As per the new alert issued on June 29th, handwritten claims received will be returned to the provider with a notice to submit a new claim in the acceptable format.
The CMS Pub. 100-04, Medicare Claims Processing Manual, Chapter 26, Section 30 notes the CMS 1500 form specifications are “required to facilitate the use of image processing technology such as Optical Character Recognition (OCR), facsimile transmission, and image storing.”
NGS currently allows for claims to be submitted online via NGSConnex. If you are currently submitting handwritten claims it is recommended to open a dialogue with your billers and consider alternatives, as many private insurance carriers look towards Medicare and Medicaid for guidance.
Medicare Beneficiary Card Changes Beginning April 2018

By: Lorna Simons, CPC
Medco Consultants, Inc
The effects of the Medicare Access and CHIP Reauthorization Act (MACRA) are rippling all throughout the healthcare community. Medicare beneficiaries will also be effected as the current Health Claim Numbers (HICNs) will be replaced. As part of MACRA, the Medicare Beneficiary Cards which use the patient’s individual social security number, will be replaced with a Medicare Beneficiary Identifier (MBI).
The MBIs will be 11 characters and alphanumeric. The new identifier will not affect the beneficiary’s benefits. The push for the new identification numbers is to safeguard patients against fraud and identity theft. Starting in April 2018, new beneficiary cards and numbers will be issued. All Medicare cards are expected to be replaced by April 2019. During the transition period healthcare providers will be able to use either patient identifier (HICN or MBI) when submitting claims until December 31, 2019.

NGS E/M Changes Not Mandatory

By: Lorna Simons, CPC
Medco Consultants, Inc
As per the June 14, 2017 News Alert, National Government Services (NGS) is no longer making the changes to the examination requirements mandatory for providers beginning 7/1/17. Providers can use either original standard or the new suggestion.

The audit tool on the NGS website will remain unchanged.
It is important to remember when documenting and coding E/M visits that they are comprised of 3 elements: The History, Examination and Medical Decision Making.
Stay Compliant When Utilizing Scribes

By: Jacqueline Thelian, CPC, CPC-I, CHCA
Medco Consultants, Inc.
With the implementation of the electronic health record more and more providers are turning to scribes to assist with their documentation. While many providers utilize scribes, few are aware of the documentation requirements.
As we are all aware, The Centers for Medicare and Medicaid Services (CMS) utilizes Medicare Administrative Contractors (MACs) to process their claims The MACs are at the local level and they have the authority to issue documentation guidelines for their jurisdiction. Therefore, you should check with your MAC for their specific guidelines.
Having said that, there are certain documentation requirements for all MACs regarding scribe documentation.
Scribes are required to be present during the encounter documenting the word and services provided by the physician in real time.
The scribes note should include:
- The name of the scribe and a legible signature
- The name of the physician providing the service
- The date the service was provided
- The patient’s name
The physician’s note should indicate:
- Affirmation of that physician’s presence during the time the encounter was recorded
- Verification that he/she reviewed the information
- Verification of the accuracy of the information
- Any additional information needed
- Remember the physician is responsible for all documentation and is required to verify the accuracy of the scribes note.
Scribe Attestation Sample:
I, _______, M.D., hereby attest that I was present during the encounter and the medical record entry for date of service ___________accurately reflects signatures/notations that I made in my capacity as M.D. when I treated/diagnosed the above listed patient /Medicare beneficiary. I do hereby attest that this information is true, accurate and complete to the best of my knowledge.
Physician’s signature_____________________________ Date: _________
I _________________________ attest to being the scribe for Dr. ______ above named patient on ________________.
Signature of the Scribe:____________________________ Date: ________
Sources:
National Government Services / Part B / Policy Education Topics / Scribes

Building Blocks of Developmental Screening

By: Melanie Thelian CPC, CPC-I
Medco Consultants, Inc
CPT 96110 Developmental Screening (eg, developmental milestone survey, speech and language delay screen), with scoring and documentation, per standardized instrument, is a commonly used code in the pediatric setting. The work and time provided by the treating provider identifies the development of the growing child. Because this service is recommended by the American Academy of Pediatrics (AAP) in providing quality preventive medicine, many physicians and/or other qualified healthcare professionals are oftentimes confused on how to document the service.
With an increasing number of commercial insurance carrier audits, requesting refunds for insufficient documentation of CPT 96110, it is important to document the full description of the code. The description of the code includes “instruments and scoring”. However, to date there is no official standardized instrument nationally recognized.
Follow these documentation requirements when providing the screening to avoid potential overpayment requests:
- Q&A on age appropriate growing an development (I.e Ages and Stages; Mchat)
- Scoring by the physicians and/or other qualified healthcare professionals
- A brief interpretation by the treating provider
- The treating provider should sign and date the instrument utilized and scan/ save in the patient’s file/chart.
Sources:
American Medical Association Current Procedural Terminology Manual (CPT) 2017
CPT Changes, 2008, Preventive Medicine Services Counseling Risk Factor Reduction and Behavior Change Intervention

Coding and Billing Chronic Lyme Disease

By: Lorna Simons, CPC
Medco Consultants, Inc
May was Lyme Disease awareness month during which celebrities such as Kelly Osbourne and Alec Baldwin described their personal stories with the disease. Though May is over, Lyme disease season continues as we get ready for the summer months.
The Centers for Disease Control (CDC) and National Institute of Allergy and Infectious Disease (NIAID) currently recommend a 2- 4 week course of oral antibiotics for treatment of Lyme disease. Many insurance carriers follow this guidance when it comes to treating the illness. This can be difficult when it comes to billing patients with continuing Lyme symptoms beyond that initial period for treatment.
The term “Chronic Lyme Disease” is a misnomer, instead the CDC and NIAID recognize Post-Treatment Lyme Disease Syndrome (PTLDS). Experts believe the symptoms of PTLDS may be caused by tissue and immune system damage caused by the Lyme disease.
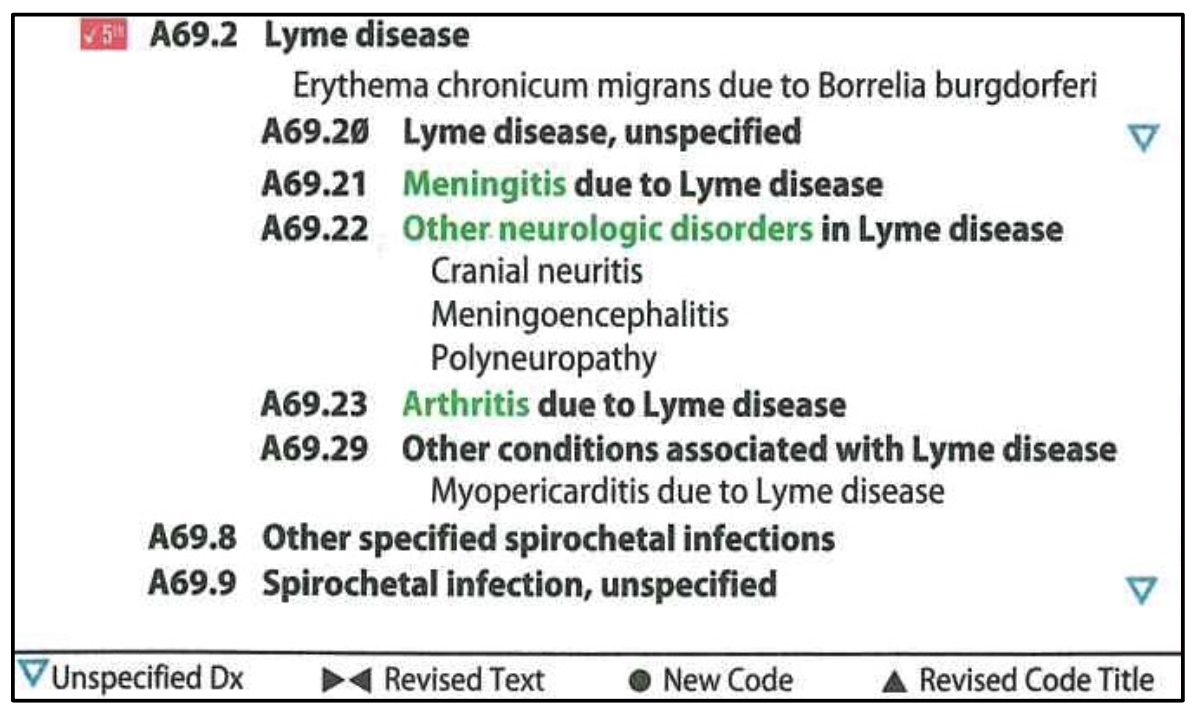
There currently is no ICD-10-CM code for PTLDS (or Chronic Lyme Disease). In the ICD-10-CM manual, Lyme disease is a subcategory with additional subdivisions. For ICD-10-CM coding of PTLDS, it would be appropriate to choose the subdivision code that most accurately describes the patient’s symptoms.
There is no current standard for treating PTLDS due to continuing disagreement in the medical community. If a patient presents with Lyme symptoms after the standard course of treatment, it is advisable to check their insurers policy for any treatment limitations. It may be necessary to provide the patient with an Advanced Beneficiary Notice (ABN) as some carriers see the treating of PTLDS with long-term antibiotics as experimental.